


Glider
-
Posts
2384 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Everything posted by Glider
-
It's been known for a long time that changes in psychological state induces changes in physiological function. That's what the area of Psychophysics studies. There's no need for spiritual or other supernatural explanations.
-
I would avoid using any invasive (skin piercing) technique at all. Unless you know exactly what you're doing, sticking needles in people is a very bad idea, particularly if you're aiming for a vein, and if you knew what you were doing, you'd know that. It's unlikely you'll get any qualified person to help you with it as it's medically unethical. If you want to fake it, then fake it. Cut the last centimetre of the needle off. Pressing the stub against the skin will, in a photograph, look exactly the same as if you'd insterted the needle. I say again: Attempting genuine venipuncture just for a photo is unethical and if you don't know what you're doing, it's a very bad idea! You have no idea of the damage you could do. DON'T DO IT.
-
You could control these urges, but it's extremely hard to do on your own, as your giving in to them demonstrates. You might learn to live with them eventually (assuming you don't seriously hurt yourself in the meantime), but wouldn't it be better to get rid of the urges altogether? You could get rid of the urges, but you can't do that on your own. I can understand why you wouldn't want to tell your parents and you don't have to. But you really should tell somebody, and prefereably, somebody who is in a position to help you. Why should you tell somebody? Because it's unlikely to get better on its own. You submit to the urge and in doing so, you are reinforcing the behaviour and so the probability that you will submit to the next urge increases. In a short time, the urges will increase in frequency to gain the same satisfaction and you'll have to do it more often. You're already opening yourself to the risk of infection each time, but also, you create scars. How long will it be before you can't bare your arms without people asking awkward questions? Not just your parents, but enybody you talk to. Do you want to have to wear long sleeves every day for your entire future to avoid those questions? I have seen the results of this many times. It's not pretty. Don't talk to your parents if you don't want to, but talk to somebody. You say you don't know why you do it. That's entirely possible, but if you talk to the right person, they will be able to help you find out. They will know the right questions that will help you to understand why you get the urges. Once you understand this, the urges will go away. No, you are not crazy, but you are fighting/punishing yourself for some reason. You have to find out why and you'll need a guide who knows the area to get there. Try to see your GP. They will help you to find the right person.
-
Yes, there is such a thing as withdrawal syndrome, but that won't make a person weak or more susceptible to illness. Not serious illness anyway. It might make a person more likely to catch a cold for a short time, but nothing more serious than that. Heavy smoking increases the risk of infections anyway, by reducing the levels of SIgA (Secretory Immunoglobulin A) secretions in the mucous membranes of the upper respiratory tract. SIgA is the first line of immune defence against environmental pathogens like cold and flu viruses, bacteria etc., so quitting will not have any notable effect in the short term. In the longer term, resistance to these infections will increase as SIgA levels return to normal but more important, the risk of much more serious illness will be significantly reduced. Addiction has both psychological and physiological components. All addictive substances, through a variety of mechanisms, share a final common effect; they elevate levels of dopamine in the reward centres of the brain. This means that the behaviours leading up to administration of the substance are strongly reinforced and so become compulsive. This accounts for the psychological component of addiction: A compulsive behaviour that will be carried out despite knowledge of the harmful effect of that behaviour. The physiological component comes from the fact that taking any psychoactive substance over time will produce long term neurological changes. In the case of nicotine (which is a nicotinic Acetyl Choline (ACh) antagonist), the body increases the number of nicotinic ACh receptors to compensate. The result is that when nicotine is withdrawn, the central nervous system is over sensitive to ACh. Nicotinic ACh receptors are abundent in the symathetic system which is responsible for arousal and fight/flight response. Oversensitivity to ACh results in the physiological withdrawal syndrome for nicotine, which includes: Restlessness, anxiety, irritability, tremor, sleeplessness. These vary in intensity between individuals. Some experience very few and mild symptomes, others experience more and severe symptoms. These symptoms, if sufficientlky severe can make a person a little run-down which might make them more likely to catch colds or other mild infections, but as I said, it's short-term. The body readapts to the absence of nicotine in about three weeks (it reduces the numbers of ACh receptors to pre-smoking levels). This eliminates the physical symptoms, but the psychological symptoms (i.e. craving, which is the compulsion to perform the behaviour) remain, albeit to a lesser degree. Such a strongly reinforced behaviour takes a lot to extinguish. Drug replacement therapy (e.g. nicotine gum or patches) is extremely effective, but not on its own. The idea of DRT is to 'take the edge off' the physiological symptoms and give the person a chance to address the psychological (behavioural) components themselves. DRT won't provide the 'hit' of reward that smoking does, but it will deal with the withdrawal syndrom so a person does not have to suffer the physical side of withdrawal. However, to rely solely on DRT just means the person is addicted to that instead of smoking. Once on DRT, the person has to change their behaviour (i.e. deal with the behavioural compulsion). Addiction behaviour, as I said, is strongly reinforced and the compulsion to perform that behaviour may never go away. Ex smokers of 10 years can still feel the compulsion to smoke (alothough they can deal with it easily). The technique is that the person has to teach themselves new behaviours to displace the compulsive behaviour, and these new behaviours have to be practiced until they become habit (unconscious and automatic), so the automatic response to a stimulus that results in an urge to smoke is something other than smoking. It sounds a lot to do, but it really isn't. The explanation is more daunting than the actual process.
-
In cases of depression, you never reach that point. There are many forms of depression and the majority have a high spontaneous remission rate. Here I thihk we're confusing plain suicide with euthanasia. If you're talking about a situation in which all other avenues of treatment have been explored etc., then it sounds like you're talking about euthanasia. On the other hand, in cases of suicide the individual, if left untreated would not die without taking their own life. If there's a life to get back, then one should try. However, in cases of terminal illness, there is nothing to get back. This is a difference between 'euthanasia' and 'suicide'. All depressed people know they are depressed, however none of them know these feeling will go away or lessen over time. It's that despair that is a major part of depression. They can know it on an intellectual level, but that's a long way from believing it on an emotional level. The intellect in these cases provides no comfort. You can know the depression will get better, but that's of no comfort if you don't believe it. That's the thing about depression. The logical triad of 'knowing' does not apply. Under normal circumstances, to know a thing, a) you must believe it b) it must be true and c) you must be justified in believing it (i.e. have some sound rationale for believing it). If these criteria are true then you can be said to know that thing. However, in depression, a person can be justified in the belief that it will pass (i.e. have a sound rationale for the belief), and that fact is true, but they can't be said to know it's true because despair prevents them from believing it. In this, they can be said to be aware of the fact that these feeling will pass, but they cannot be said to know it. Whilst depressed people are not insane, they have lost their perspective and are only 'seeing' half of reality (the negative half) and so cannot be considered to be of sound mind. To accommodate their suicidal wishes is not helping them at all, it's buying into their belief that their despair and loss of perspective are permanent, which is not true. I don't think you can ethically provide euthenasia based on a false premise. The difference here is what the patient has to lose. The terminally ill patient has nothing to lose. The depressed patient has the rest of their lives to lose. Their not wanting to live it is a temporary state and the best you can do is help them through it.
-
He must be a King! He ain't got sh*t all over him.
-
You mean Multiple Personality Disorder (MPD).
-
I should have been more clear here. Depression is always treatable yes (insofar as depression can always be treated), but that doesn't mean the treatment is always successful. I was using the term 'treatment' in the sense of 'an intervention with a good probability of success'. In more severe depressive conditions, (e.g. bipolar disorders), the condition may not respond to treatment per se, but it is controllable, i.e. the intervention (e.g. lithium) does not 'cure' the underlying condition, but will control the symptoms. So, whilst depression is always treatable, the treatment is not always fully effective, but under those circumstances, what's left is controllable. Arguably yes, but only if one is arguing for the right of suicide which, I think is qualitatively different from euthanasia. Given that in so many cases, depression is temporary (it may be long-term, but that doesn't make it permanent), I think it would be a mistake to provide euthanasia for depressed individuals. Revcovery rates in depression are usually good, but the problem is that due to the nature of the condition, insight and perspective are the first things a depressed person loses. This is evidenced by the fact that every week in the USA, a doctor commits suicide (not the same doctor), even though they are in a good position to know that the condition is potentially treatable or self-limiting. I think to provide euthanasia to somebody who is known to have lost their insight and perspective would be wrong. As to whether they have the right to commit suicide nonetheless, that's a different discussion.
-
Not really. That would make the entire euthanasia discussion a catch 22: If you express a wish to end your life, you're clearly not sufficiently competent to make the choice simply by virtue of having made the choice. This is quite a common argument against the right of a patient to choose to die, but the problem is, it's expressed as an abstract logical argument, completely free of context and situation (i.e. as if preceded by 'all other things being equal'). Under those circumstances it has validity (at least, face validity) and runs thus; in a healthy person about whose future it would be unreasonable to predict a significant deviation from their current state, the expression of a wish to die can be seen as unreasonable and thus indicative of an abnormal psychological state. However, expressions of a wish to die rarely come from healthy people and when you add context, things change. In a person who through some pathology is experiencing severe intractable pain and suffering and whose prognosis is more suffering, the loss of their faculties, their dignitiy and humanity and eventual death, the expression of a wish to die in order to avoid that process is quite reasonable. There are things worse than death and I think the expression of a wish to avoid them by choosing to die a little earlier suggests a normal, reasoned response to an unusual situation. I think the biggest problem comes from people who simply cannot imagine themselves ever choosing to die. This, by extension suggest thay cannot imagine themselves in that situation (i.e. they lack empathy), which, I would suggest, disqualifies them from making decisions on behalf of the individual who is in that situation.
-
I'm for it. I believe in the right of the individual to choose the time and mode of their own death, but I'm talking from a clinical standpoint, which means I'm referring to patients in severe and intractable pain from terminal conditions and not advocating people throwing themselves under trains because they're depressed (depression is treatable). The forms of euthanasia listed in the OP (passive Vs active) are not quite accurate. The levels are passive, non-agressive and aggressive. Passive euthanasia is already quite common. This involves the withdholding of medication or treatment as in DNR orders (DNR = Do Not Resuscitate), or the necessary administration of narcotic analgesia at levels that, although required to control the pain, will kill the patient (in this case, death is the by product of the necessary analgesia, not the objective). Non-agressive euthanasia refers to the withdrawal of life suppot mechanisms (ventilators, dialysis etc.) and agressive euthenasia refers to the application of a substance (usually an anaesthetic) where the objective is death. In all cases, it should be borne in mind that the term euthenasia means 'good death', i.e. a dignified and pain free death by personal choice rather than being forced to linger on in protracted and intractable suffering because it is against the principles of those treating them to allow (or help) them to die.
-
Not placebo, but are sure it was the WD40 and not the rubbing it in that helped?
-
Yeah, a lot of cults take that approach: 'You're either saved or damned', 'You're either with us, or you're against us' and so-on.
-
Dude, only 1 cup of coffee, it's not even light out yet and you want perfection? Anyway, I was using Latin rules of syntax But that's the whole point of A-Levels, so tutors in higher education can assume a certain standard and not have to waste time with remedial teaching of stuff that should already be understood. True. I don't think it's over the top. Schools may be lowering the bar for written English, but scientific journals are not. Ultimately, graduates should be able to write at a standard that would be acceptable for publication, but it's getting harder to get them to that level as they are entering HE with lower standards to begin with. I think students rely too much on spell checkers and other automated tools and not enough on proofreading. To a spell checker, "Dear Sir or Madam" and "Dead Sod or Moron" are equally acceptable.
-
I never used to care about it really, but so many school-leavers entering University such have crap writing skills that we find outselves having to go over these basic things again and again. It takes up a lot of time that could be spent on other, more relevant things and it starts to grate after a while. I'm not really concerned with perfection, but basic things such as those mentioned in the first five posts. We are supposed to be able to take a certain level for granted in A-Level students, but it seems to be getting worse. I've even seen SMS shorthand appearing in essays over the last few years (4 example, & just so u no), it gets really annoying.
-
Aargh! Or 'Amount' Vs 'Number' as in "The amount of participants tested..." The first set of marking is due in soon...I can't bear it! Ahh...tautology, another favourite. Either 'apostrophes that aren't used properly' or 'that aren't used correctly' is adequate. The use of both, as in '...that aren't properly used correctly' is a tautology Yeahuh, but you lit the fuse when you raised something that bugs so many people
-
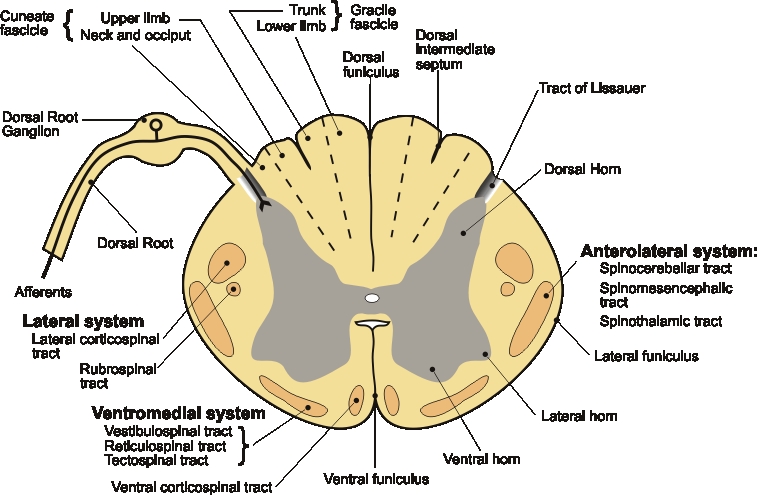
The large sciatic nerve is comprised of a collection of a number spinal nerves that project from the L3 to S1 roots (compression of each gives different symptoms, but all are classed as sciatica), but there are 31 pairs of spinal nerves (i.e. 31 on each side of the spine). Each spinal nerve contains both afferent and efferent nerves, which enter and exit the vertibrae via the dorsal and ventral roots (respectively). So, there are 31 pairs of dorsal and ventral roots from projecting from C1 to CO. The dorsal roots have swellings (ganglia) because they contain the cell bodies of the unipolar afferent neurons. The ventral roots don't have swellings because the cell bodies of the multipolar efferent neurons are in the ventral horn of the spinal cord. So, the dorsal root ganglia are simply the swellings (collections of cell bodies) that can be found in any of the 31 dorsal roots.
-
Hey Fred56: The nerves entering at the dorsal horn are Afferent (sensory). Efferent (motor) nerves exit via the ventral horn. As you say, there must be a path all the way to the brain, and most sensory pathways are three neuron pathways. The axon branches of the first neuron is tipped with sensory 'organs' (pacinian corpuscles, ruffini endings, Meissner's corpuscles, free nerve ending or whatever). The axons of these unipolar afferents go from these endings, all the way to the dorsal root at the spine, where the cell body is conected to the axon by a single projection coming sideways out of the axon. These afferent cell bodies collectively form the the dorsal root ganglion (the swelling in the dorsal root). The axons, once past the ganglion are technically dendrites, but really, they're just the part of the single fibre that exists after the somatic projection. These continue on into dorsal horn of the spinal cord, where they synapse with large spinothalamic projection neurons. It's a bit more complex in that there are interneurons and things involved, but primarily, these first afferents connect the periphery to the large spinal neurons in the CNS. Spinal projection neurons (mainly spinothalamic, although there are other large tracts in the spinal cord) project from the dorsal horn of the spinal cord, to the thalamus (lateral and medial thalamic nuclei) travelling up the dorsal white matter of the spinal cord (cuneate and gracile fascicles). All sensory information (except smell) passes through the thalamus. From the thalamus, shorter projection neurons carry the information to appropriate parts of the brain; primary somatosensory cortex and so-on. So, in most cases, sensory pathways consist of only three neurons: From the periphery to the spine, from the spine to the thalamus and from the thalamus to higher CNS areas. I've attached a slide showing a transverse section of the spinal cord to give a better idea. You can see the afferent enter the dorsal root, how the cell bodies of these unipolar neurons form the dorsal root ganglion and where these neurons synapse in the darker area of the spinal cord at the centre (darker (grey matter) because it contains large numbers of spinal projection neuron cell bodies) and the lighter (white matter) tracts that form the cortex; dorsal ascending pathways and ventral descending pathways. The ventral roots (not shown) contain the efferent fibres that project out to their respective effectors.
-
Can we have one on 'your - you're' and 'their - there - they're' too? (or is that 'to?')
-
Always a good tactic. Sorry I blew it for ya
-
Peripheral neurons are longer. The spinal cord is only about 45cm, but the snsory nerve that runs from your toe (for example) to the dorsal horn in the spine is longer (can be >1 metre).
-
Yes, ergo = therefore and sum = I am, as in 'Cogito ergo sum'.
-
I think an important point is that if a conscious person catches fire, they tend to then try to put themselves out. In most reported cases of 'spontaneous human combustion', there are no signs of this effort, which would suggest that the individuals were not conscious at the time (and thus not moving around to generate static and were quite well earthed), which, I think, puts a different slant on possible events leading up to death. Particularly in those who smoked.
-
I won't According to the Freudian model, babies and infants are mostly ID (which is said to be based on the pleasure priciple). Their immediate wants and desires are the most important and must be satisfied first. This is obviously necessary in babies, but infants and toddlers do it too. They'll quite happily override anybody else's needs or wants to achieve their goals, e.g. they're quite content to disrupt an adult conversation or activity with loud demands, or scream in shops "But muuuuum!! I WANT IT!!!" As they grow (the model states) they develop their super-ego, which is the socially acquired conventions. The ID and ego are internal, whereas the super-ego is externally acquired, The ego moderates between the ID and the super-ego, as I say, balancing between the demands of the ID whilst conforming to social convention. Well, the answer is really in your post. As you say, the ID and ego represent the unconscious and conscious and are thus both internal. The super-ego is external and has to be socially acquired and so is different between individuals according to culture (whereas the ID and ego are the same between individuals). Having said that, I don't believe any of it either. I'm not arguing for the existance of the ID, ego and super-ego, I'm just clarifying the Freudian model (in the same way that clarifying the Arthurian legend might make people's understanding of the legend more accurate, but doesn't make the legend more true). The ID, ego and super-ego 'legend' was proposed as one 'model' of how things work, but it's not testable nor observable, i.e. the purported stages can be observed, but the ID, ego or super-ego per se can't be, nor can their alleged effects. As far as they go, I think they're really just arbitrary labels naming stages of development and you might just as well call them 'Colin' 'Julie' and 'Steve'. There are better explanations for the relationship between basic internal drives and the development and learning of social rules and behaviour. I don't think readjusting the Freudian model by eliminating the super-ego or shuffling the elements around makes it any more useful or true.
-
That's the super-ego. In classic Freudian terms, the ego moderates between the ID and the Super-ego, trying to find the balance that most satisfies the ID, whilst conforming as much as possible with the social constrictions laid down by the socially acquired super-ego.
-
To remove waste products from the blood by filtration (takes place in the renal glomeruli in Bowman's capsules found in the renal cortex), and to control body fluid levels/reclaim water through osmosis using a sodium gradient (takes place in the loops of Henle which form the renal medulla). As renal function is dependent upon blood pressure, the kidneys are also involved in controlling that. The kidneys also produce erythropoietin (EPO) which stimulates red cell (erythrocyte) production in bone marrow, which is why patients in renal failure need to take EPO regularly. So, main functions: Blood filtration, regulation of water in the central compartment (circulatory system), regulation of blood pressure, regulation of red cell production.