CharonY
Moderators
-
Joined
-
Last visited
Everything posted by CharonY
-
I actually don't know whether there is good data on it for humans. In rats, N2 is not considered an effective means of euthanasia (whereas CO2 is allowed, mostly in conjunction with a secondary euthanasia method). In rat studies, exposure to 100% N2 induced hyperreflexia (twitching) and unconsciousness after 3 minutes and death took over 7 minutes (30s and 2.5 mins for CO2 no twitching, reduction in heart rate and respiration). There is also a higher risk that animals recovered after assumed death. I would think that a method not considered suitable for rats would also not be considered suitable for humans.
-
Well, it is a question what is being measured, isn't it? There is the concept of the savant syndrome, where folks can perform astonishing tasks in one particular area. Others do not excel in any one area but have massive breadth. That all being said, I think the biggest factor for any smart brain is training.
-
Doesn't even need to be a specialized forum. Being unashamedly uninformed is the new cool.
-
I think when it comes to infections, it is generally more accurate to refer to treatment, rather than curing. Generally speaking, treatments aim to reduce viral load and/or supplement the ability of the immune system to do so. Antibody-based treatments can be vulnerable to mutations, but not necessarily so. Paxlovid contains an inhibitor for a viral protein, which reduces the ability of the virus to replicate. Mutations in the gene encoding that protein could reduce effectiveness, but it is still very effective in preventing death. It is important to note that treatments are not binary. They aim to reduce viral production and accelerate clearance. Depending on when you start taking the medication has therefore a big impact on what is happening to your body. Short incubation periods (which suggests high levels of replication of the pathogen) can make things difficult, for example. Which is why vaccinations are so effective, as they basically prime your immune system to do the same thing as a treatment would. The main limitation is that the fast response (via neutralizing antibodies) drops over time, but the secondary (i.e. memory-based) response still kicks in. So basically the best "cure" as in not getting (seriously) sick is still being up to date with vaccinations.
-
The thread is old and doesn't make a lot of sense, but the helix is on the DNA, nit chromosomal level.
-
I have not checked it, but I think there was a Legere poll that had it broken down more. I also just saw a poll in Germany (from 2020, so things might have changed with the AfD getting so popular) where about 89% were in favour of Biden and 4% preferred Trump. I hypothesize that stupid is in fact contagious and driven by proximity.
-
First, it does not edit genes as such. It can be exploited for such purposes (in biology, we have a long history of using cellular enzymes for genetic work), however in nature it basically just recognizes foreign (viral) genetic material and just degrades it. Second, there are other enzymes, such as recombinases that can integrate foreign DNA into its genome, as well as other mechanisms that prevent it (e.g. restriction enzymes). But even our usual DNA replication system that tries to copy without errors, does, in fact eventually introduce errors, which creates mutations. In other words, there are a lot of things that can alter DNA (internally and externally) Here, you have to go back to the hierarchies that I a referred to earlier. On the mechanistic levels a lot of thing manipulate genetic material. Either by making errors or allowing errors and so on. Their impact on evolution is not zero, but rather it affects the overall genetic landscape in terms of e.g. expected mutation rate, potential role of horizontal gene transfer and so on. However, when it comes to the mechanisms of evolution, e.g. selection, the same rules apply as for any other traits that a cell or organism might have. So if you have cell that is very promiscuous with gathering foreign DNA (e.g. it does not have restriction enzymes and has a highly active transformation system), it could get lucky and get DNA from the enviroment that is highly useful and it will be positively selected. Conversely, it might get a lot of useless DNA which just cost energy to replicate and then its fitness will go down. I.e. you should not think too much in terms of yes/no but rather on which level and how much. If something impacts genetic material itself, it can affect certain overall parameters (again, mutation rate being the most obvious ones), but beyond that, it does not have a particularly different role. Depending on environment, these might be very important. For example, in an environment with a lot of viruses/phages, having CRISPR as protection might be very important. In other environments, it may be much less so. I think we have to be a bit more precise. Luckily, I think we have moved away from the idea of guided evolution to a large extent. But now that we have arrived at a somewhat better place, I think absolutes are not really helpful. CRISPR is an enzyme complex as any other and proteins obviously do have functions, leading to traits, which might then be under selection. So thinking that CRISPR somehow changes the course of evolution single-handedly is clearly not what is happening (if we ignore artificial breeding for the moment). Because at that point we might as well argue how dead we all would be without, say, ribosomes which I think is not terribly helpful (though there is a reason why they so conserved).
-
Pretty much that. At least in the given context of understanding the basics of evolution. It is interesting for the specific question of the evolution of arms race among cells and viruses. There are a lot of them around, including the very long-known restriction enzyme systems, which bacteria use to degrade foreign DNA or the range of weapons that bacteria use against each other. It all makes sense from the viewpoint of a selfish gene (though that itself is a simplified narrative, of course). It doesn't change the overall system. It is just one of many existing traits (or virtually all traits) that exist. You could say the same for virtually anything in a cell from polymerases to ribosomes. CRISPR is nothing extraordinary in that regard. You see a lot of it around in press, because it is useful for biotechnological applications but so are polymerases and restriction enzymes. They are just much more established and therefore less showy.
-
I think you have to be careful when thinking about randomness in evolution. In fact, there are multiple levels to think about it. First, is the mechanisms which create diversity. They include mutations, recombination and associated mechanisms. They are mostly random for most intents and purposes, but looking deeply into it, there are certain chemical reactions resulting in certain mutations that are slightly more likely than others, for example. But the likelihood that they are happening at all, are mostly stochastic. Then, you have the mechanisms affecting the inheritance of genetic material. Here, we clearly have random effects (e.g. drift) but also non-random mechanisms (e.g. selection). Finally, we also have the overall view on evolution. The important bit here is that because of potential strong effects of selection, evolution is not an entirely random walk. However, the measure here is fitness (i.e. ability to transmit genetic material to the next generation, not fitness in the physiological or survival sense). But fitness is highly context-specific and depend on the organism and its ecological niche. So while not random, there is also no clear goal, either. Going back, things happening at the First (lowest) level, do not have systematic impacts as such, they are one of many traits that affect the impact the system in terms of e.g. how fast new traits might appear, but they work in conjunction with myriads of other factors affecting traits. Selection, on the other hand, works on a higher level and takes the combination of traits, in a given ecological situation and there impacts the gene pool systematically, if you want to call it that.
-
I don't think that question makes a lot of sense without further context. Chromosomes can increase in length rapidly due to integration of other DNA (e.g. horizontal gene transfer) and it can also get pruned quite massively. Some organisms (usually simpler ones) have expanded their genome size massively (some amoeba have around 200x of the human genome). Others, such as parasitic organisms, have lost a lot of DNA and have a very compact size. I.e. there is no mechanism that I am aware of where we would expect a constant expansion over time, if that was the question.
-
Yes sorry, brainfart. 67 Trump would have been... bad. Well, worse.
-
This is how it can work, but the key purpose is to prevent or at least reduce serious events. And so far, the only vaccine drive that managed to eradicated a diseases was for smallpox. Issues with administering or resistance to getting vaccinated have caused a resurgence of a range of diseases that have been near extinction. Similarly polio has been circulating for a while in New York, for example. Math is hard, I get. If 80% of the population is vaccinated and in a pool of fatalities you find that 58% are vaccinated. Is that high or lower than the expected rate, if vaccines had no effect?
-
I have seen another poll which was phrased differently, but ultimately I believe highest support was age dependent, with highest support among younger, then dipping, peaking around 40s, then declining.
-
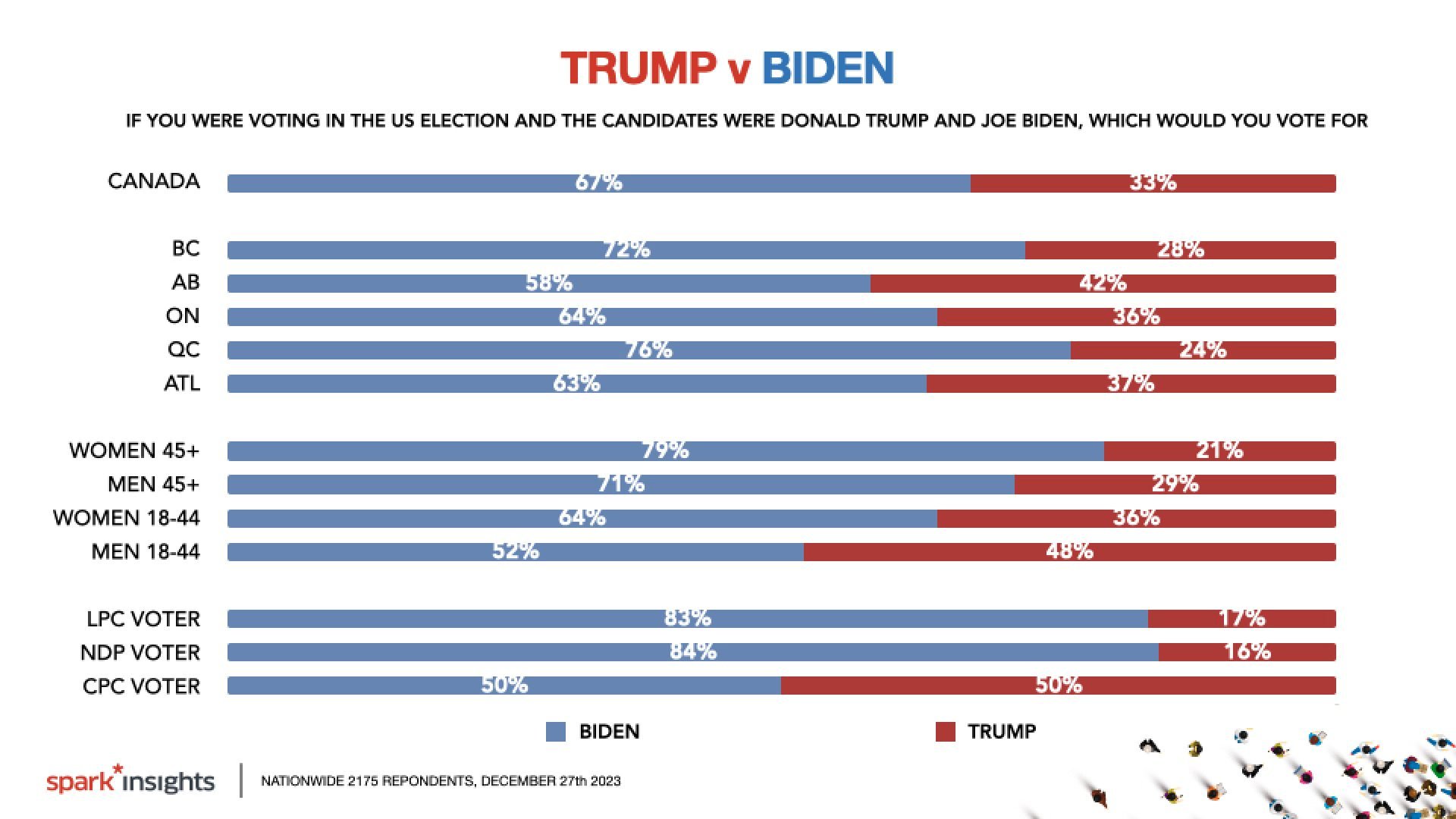
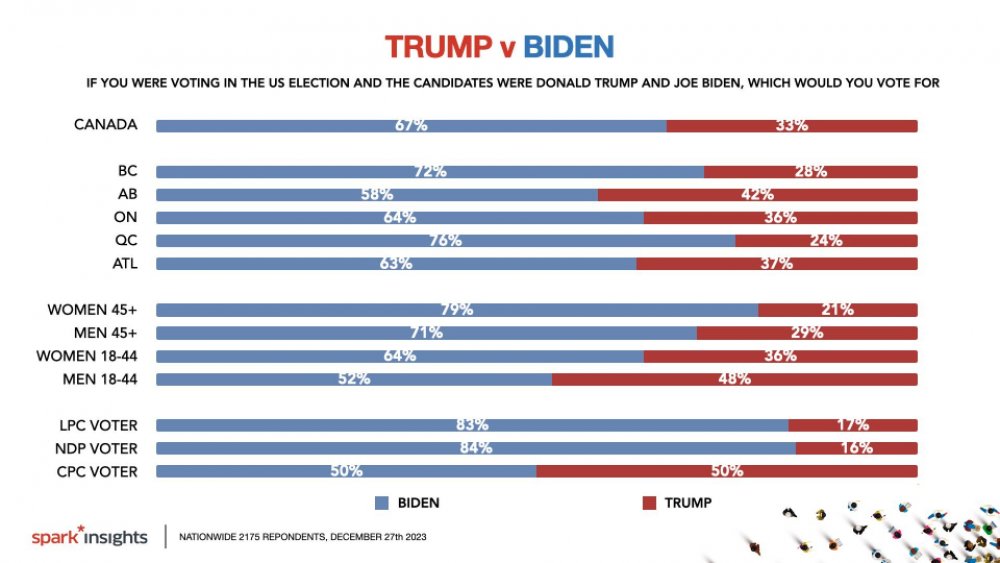
Just a little something from Canada, when asked who they would vote for, if it was between Trump and Biden. It is still 33%, who would vote for Biden, with an even split among conservative voters (and close for younger men).
-
Poor math and reading comprehension it seems. I.e. forgetting that more than 58% were vaccinated (i.e. the rate of deaths in vaccinated folks is disproportionately lower) and just a few lines further in the article it is even explained that the unvaccinated folks were at over 8-fold more likely to die. While not tangential to OP, it suggest that the poster has a habit of either being very uninformed and/order argue in bad faith, as they obviously do not even read what they are linking.
-
Theere should be. I remember a study around 2000s that measures task switching as a measure of focus of around 2.5 mins. A recent follow up from same author measured around 0.5 mins or so. I have the papers... somewhere.
-
That is true and exactly the problem. For example, attentionspan and is going down everywhere, but it is not clear whether current tests account for them.
-
There is that, but I think with more data, we are starting to think a bit more about what is the range of normative behaviour? At which point does a certain behaviour cause dysfunctionality and requires additional treatment and how is what we should accept as normal range? One big issues is that in contrast to, say, infectious diseases we do not have causative agents, or even absolute clear targets. I am fairly sure that among experts, there is a more nuanced discussion about that, though.
-
Also note that it is easy, especially non-quantitatively to correlate two or more random temporal trends with each other.
-
This is a bit of a discussion going on, and goes beyond textbook knowledge. I.e. the questions there are not clearly resolved. There are certainly proponents stating that we have overlooked their importance for too long, and there might be something to it. Others might argue that the importance might be overstated as existing models seem to deal with overall questions fairly well. It is not my field, so I am certainly not familiar with all the intricacies (and my knowledge is also somewhat dated) but my reading when things came out was that yes, there is likely an influence, but given all the other aspects that are already known to play a role, it looks more like an addition that one has to acknowledge only in certain models. That being said, I believe there is more lit out there specific regarding plants, but as I am not a plant person, I have no insights about their significance. That all being said, if one wants to start about the basics of evolution, one should start with the basics before exploring more complicate advanced topics. Inevitably, starting off the other way round will lead to misunderstanding and confusion.
-
Cooking is just applied biochemistry.
-
What you are talking about are generally not related to evolution as they occur only within the organism and are (generally) not transmitted to the next generation via the germline (there is evidence for some exceptions, though). In broader terms, it is important to note that DNA itself is not doing anything. Simplified, their main role is a data repository that needs to be first transcribed into mRNA and then translated into proteins. The latter are doing all the work. Obviously our cells (and by extension our body) need to be able to address changes in the environment, each cell type has to fulfill different functions despite all having the same DNA. So what is happening is that transcription/translation is regulated via a wide range of internal and external cues resulting e.g. different protein compositions in different cell types or adaptive changes in response to some environmental signals. However, this dynamic is within an organism and is not transmitted to the next generation (e.g. in a Lamarckian sense).
-
Also, yeast extract is typically used for flavoring. It is a cheap source for umami.
-
There is an even worse implication. If impeachment is a prerequisite, it means that the president could avoid all criminal liability by simply resigning (well or killing everyone who would vote for impeachment).
-
Not necessarily in that granularity but there are studies looking at it. https://doi.org/10.1093/pnasnexus/pgad318