

CharonY
Moderators
-
Joined
-
Last visited
Everything posted by CharonY
-
I disagree, not fully but some extent. The pendulum is moving and the issue is that it is a bit unclear if we know where to stop it. There are some isolated papers who are excessive, but they pale in contrast to the existing body of lit of strong narratives. But the egalitarian spin is not the claim that everything is socially constructed, especially if you read the papers carefully. Rather, the claim is that the social overlay is so strong, that you need extraordinary amount of data from several disciplines (and not just a simple measure as per Rushton, Jensen, Lynn and others, who are all psychologists but try to make biological arguments). I.e. the former assumption was basically everything is pre-ordained by evolution and dominated by genetics. However, biologists have moved away from that quite a bit quicker than some areas of social sciences, after realizing the complex interplay between genetics and the environment, even on the cellular level. Regarding SNPs, you wouldn't need to know which are associated with intelligence if you use GWAS methodologies. If the basis is some hidden genetic pattern, you should be able to delineate high-intelligent from low-intelligent folk across all socioeconomic and racial groups. That attempt has failed. Regarding twin studies, in order to separate out environmental factors you would need to separate twins and e.g. have one placed in a developing country and another in a, say rich household in a developed country. Those studies have small cohorts and almost always have children originated from poor countries (adopted into a developed one), that is already being under potential harmful influences and I don't recall studies with the reverse setup. There are studies however, that have shown that heritability in twins can vary which indicates that development is not fixed. But again, there hasn't been really an argument that IQ has no heritability (which is a slightly different argument whether certain genes are associated with higher IQ, as it measures generational transmission and cannot really make a functional association), but rather the relative role between genetics and environment. You forget the single most important element: the plasticity of the brain. Even if if we found a genetic pattern that is directly and clearly responsible for high IQ, take this child and rear it in the dark with no social input. It would not only do badly but utterly fail an IQ test. The point is that there is still discussion an what the psychometric measures really measure. The good thing is that some seem to measure something stable but there is a broad discussion about what they mean. And we are not even touching the biological aspects of it. And then there are the limits of natural experiments where you always slice and dice cohorts. And finally, looking at genetic traits that can bring advantages the big questions is how and how they are distributed. Assume that there is a set of genes that make you very good at reading (say some sort of pattern recognition and recall). In a setting where reading and writing is common, that person might excel in written tests. However, the same trait in a hunter society may also be of benefit, such as for hunting. Yet, if illiteracy is the norm it might never translate to written tests. And even if folks apply a culturally appropriate test (which in itself if problematic) they might do it verbally, a test for which those genetic traits suddenly do not provide a benefit anymore. From a biological point of view, the issue is fairly obvious, traits only manifest themselves by interaction of the molecular machinery (which adds flexibility to the genetic underlining) with the environment. It is always both and there are scenarios one or the other contributes more. These shifts tend to be dynamic and require a lot of work to untangle, even if we just use cells. To me it was always baffling that folks think that they can make strong theories and assumptions on the vastly more complicated, much vaguer and much less well understood concept of intelligence (and not to mention the issue with defining racial boundaries on top).
-
And work from the same authors will dominant in the first couple of your searches (e.g., Rushton, Lynn, Jensen). And there is a reason for that. It is also important that these resurgences of eugenics line of thinking happened when the "big narrative" type research saw an upswing, which includes the rise (and eventual fall) of disciplines such as sociobiology and evolutionary psychology. Lack of reproducibility and inability to resolve cofounding factors ultimately challenged the disciplines wholesale. I would suggest to follow up your reading with folks like Nisbett, Wicherts and I think Litman for very extensive critiques to issues ranging from methodology to poor reproducibility. There have been quite a few on GWAS and IQ, but the one that I was thinking of, specifically looked at that in a racial context. Other studies have found SNPs that are associated (if frequently weakly) with educational attainment. If the genetic link is strong, techniques like polygenic techniques should be able to estimate heritability of such a trait. Estimates from those GWAS found that maybe around 10ish% of the variation in certain intellectual measures could be explained by genetic differences. There are similar studies looking similar and different sibling groups, trying to account for the environment (published by Lee et al In Nature Genetics, I think maybe around 2018). The follow-up I am thinking about used similar techniques to specifically look at black white divide and found an even smaller impact. I think it is suffice to say that the stated premises are very much mired in the findings of some influential groups around the 90s and still have some proponents, but the cumulative work of many more folks have failed to validate those claims.
-
There is something I think called the Nobel syndrome, where Nobel price winners go off on the deep end once they get it. Curie was a notable exception (as she went on to win a second price, instead). But I also meant that hi grew up in a different time, where gender and racial differences were just accepted as facts and are therefore less inclined to review information that counters it, as a good scientist should. The issue is often that scientists might inadvertently provide credibility to such notions, though they are way outside of their expertise. As I mentioned before, Rushton (whom you seem to cite here) has been pretty much outdated and he created a body of literature who tried to link IQ with race. It was fairly prominent in the 90s I would say. A key issue even then was that he was a psychologist and tried to invoke biological concepts (such as reproductive strategies) which he clearly only poorly understood. His contemporaries already questioned some of the results based on their own studies (there has been a quite some exchange with Nisbett, for example). And in the later works Rushton increasingly seemed to slice and dice his data to accommodate his view while dismissing other studies, which created some bad blood with his colleagues. There is a huge spinoff, many questioning suitability of standardized IQ tests in various contexts (there was a paper from Wicherts discussing it in the Sub-Saharan context). The long and short of it is that certain psychometric measures considered to be universal, are not. Only once certain environmental components are fulfilled (e.g. nutrition, basic schooling, stable environment) do this measures become comparable. One especially strong correlated was also found in vocabulary development (which in turn is associated with education). In multiple studies using IQ test without vocabulary tests the IQ gap pretty much vanished (studies from the 2000s). But even some of the basic assumptions you have mentioned are not quite correct. For example: I believe that is what Jensen and/or Rushton have repeated in their papers. Yet in Flynn's work back dating back to the 90s have already talked about the diminishing gap, which Rushton later tried to argue away (which in turn lead to a whole slew of related discussions). The point is that Rushton's work keeps cementing a hard delineation, something that is not found by most other researchers and, importantly, makes little biological sense, from our understanding of population genetics. Even if disregarding ongoing gene flow, Rushton's hypothesis was delineated among black as the lowest racial IQ group, whites in-between and Asians the highest. Yet, studies have shown that folks closer related to the Asian's, such as Indigenous Americans, as well as Asians with low socioeconomic status, have similar scores as black folks. So from first principles, the biological argument was already weak, but there was a fairly recent work (I forgot the author, but could dig it out) using genome wide associated studies based on the 1000 genomes using a range of cognitive tests have failed to find any genetic links. Ultimately there is a huge body of lit that disputes this rather old claim, bolstered by improvements in our understanding of genetics. On the other side, we have Rushton and a few other researchers who not only claim a racial element, but even a hard racial delineation, essentially re-using their own arguments they came up with, when we knew less. Reviewing the full body of literature, this hard delineation is simply not supported and should at this point (or really, since around 2000) should not be taken as fact. It goes a fair bit into old men's pet theory territory (and I know a fair bit about old men and their scientific theories).
-
The critical bit is the second half, where he adds that all testing suggests otherwise. And he added that people who deal with black employees would agree. He also reiterated in various other places that IQ differences between black and white folks is genetic. Watson has at various points endorsed the book by Rushton and Murphy (which suggests strong genetic differences between white and black folks, in a range of parameters ranging from reproduction, physical strength and IQ, all of which have been refuted by broader studies). I think part of OP is that Watson had strong beliefs regarding racial differences, which ultimately are not sufficiently supported by science but has detrimental effects if assumed to be true regardless. For many, this is at least one element of why Watson was considered controversial (plus a host of other elements). I think much can be attributed to being an old man, and whether one considers that as an excuse or not is a different issue (there are other old men who have been much better at following the science and treating their folks better).
-
Well that hypothesis is easy to test and the latest analysis on Neanderthal DNA has shown a gradient from west to east. I.e. while east Asians do have higher levels of Neanderthal DNA than Sub-Saharan Africans (on average), they are also lower than in Europe (on average). So if that was a driver for IQ scores, you would expect highest levels in Europe (and likely lower in white populations elsewhere due to increased intermixing).
-
What when did that happen? Last thing I heard he was Harvard's president and only resigned recently from that position (not sure if he is teaching), because of his association with Epstein. Nothing about that the story says "poor man" to me. And I do find it highly controversial for suggesting that someone with a certain skin color is destined to be an underachiever plus a long history of abusing female postdocs who he did not consider first tier, yet not doing so with male postdocs of the same caliber. As someone with power over other's careers, this is highly problematic. The key factor here being genes isolated from gene flow. Most studies have shown that populations found in a geographic location, regardless of superficial features such as skin color are highly mixed. This is why data suggests higher diversity within such groupings than between. Geography and gene flow are determining factors, and the correlation of such groups using such high-level features such as skin color just doesn't work. Except they arent' in isolation. In the US life outcomes are not only correlated with skin color, but even more so zip code. I.e. the social and socioeconmic background is the biggest factor for many elements that we can measure (including biological parameters, such as life expectancy). It just so happen that these are also co-correlated with skin color. Yet if one were only to look at the genetic level, and fully ignore things like socieconomic status and skin color you won't find markers that are associated with high intelligence which are enriched in white or Asian populations. That is not to say that there is no genetic component, but the issues range from the measurement itself (either IQ or g, which have different methodologies) to identifying potential genetic markers and then the assumption that they are not only correlated with certain populations, but somehow these populations also correlate what we superficially consider to be "races". The latter being historically coded by a weird mix of skin color, but also some moral/social determination (e.g. Obama considered being black, which obviously does not fit his actual heritage). Fundamentally one can make it easier, most human populations, especially in modern times are mixed so patterns should are really expected to emerge in highly isolated groups which tend to have low genetic diversity (say, Amish, or uncontacted Indigenous group). In virtually all other groups the idea that skin color or similar features are genetically deterministic of things fails to yield reproducible results. Anyone working on genetics should know that by now (though to be fair, Watson was a biochemist and not a biologist). More importantly, it is not a good indicator of genetic composition, virtually all populations are patchwork of sorts. Black folks in Brazil are for the most part closer to white folks in Brazil than black folks in the US, for example.
-
It depends really, we have had multiple discussions on this forum regarding IQ. There are multiple issues ranging from what IQ really measures, which is not entirely clear, given that it was initially developed to detect deficiencies and not as much as a scoring something on a hierarchy. An associated with that, we have seen first a rise of IQ over the years (Flynn effect) but more recently the reverse was observed, especially in developed countries. Given these and many more issues, population-wide averaging of such psychometric measures and drawing conclusions from them are hugely problematic. They depend a lot on how a given test cohort was formed and there are many cultural elements regarding formats. Folks like Rushton and Murphy largely overlooked such details to spin out there big narratives and this where the controversy (and bad science) resides. In a way it is another story of a big leap of ideas, only one that turns out not be substantiated independently.
-
Except they didn't. Their paper really did not add any data. It was explicitly written as a model proposal and as far as I recall they only vaguely indicate that their model is based on some data, while acknowledging that independent verification is needed (or something to that extent). There have been different narratives on how that paper came to pass, but in one of them both basically fiddled around with models to try to see what fits the existing information. At that point however, both A and B forms were likely and some of Franklin's data pointed more towards A, which makes sense, as it is more ordered and more likely to occur during the crystallization process. I think Watson at some point also commented that he was luck not to seen Franklin's full data set as it would have undermined his model a fair bit. And that is what Franklin was doing- proposing multiple models in alignment with her data. Watson pushed one more but not based on existing evidence or further confirmation. Jumping the line, so to speak. Or ego. After all, people tend to forget all the times you were wrong and if your ego can take it, more power to you. I don't really think so. In some ways yes, but only in fairly recent times. That statement likely was based on the horrible book "The Bell Curve" a rather controversial book that tries to make a quasi biological argument for race. In most serious areas of genetic and related research it has been severely discredited (and serves as a cautionary tale if folks like e.g. psychologists extrapolate things in other disciplines based on their own).
-
Not only providing the data, but a careful interpretation of the precise elements of it. This is, unfortunately very common. A researcher I worked with, which is a powerhouse in the area of crystallography had similar stories about her advisor, whose career was built significantly based on her "fiddly" work with advanced their field significantly. Based on the stories, he was aware that, too, a he took her in as a postdoc, but torpedoed job offers she got for faculty positions. To some degree, yes. But in sciences it lagged quite a bit behind. I am fairly confident that in the 60s the issue persisted. Mayer, who won a joint Nobel was delegated to a research assistant for much of a career, despite advancing the field significantly. That being said, to me the sexism is just an addition to the story, I very much prefer a careful investigation and analysis of generated data, rather than presenting the most exciting and attention-seeking one. I will add that coming from the experimental field, I am of course somewhat biased. But even theoretical models tend to have to pass either independent validation or have some sort of mathematical proof. Eh, the economy was rebuilt before the crash. And Hitler's recovery was built on war economy deficit spending, which is not really rebuilding but just taking on a huge credit with the hope of making the occupied nation pay. In Watson's case, at least from my point of view, Franklin's paper was much better as it more closely followed the available data. At least from my reading I see two papers, one loud and brazen and the other careful and meticulous. Yet only one gets all the credit.
-
I disagree. Every scientist has pet theories in their field of study. Most of them will turn out to be wrong and some will happen to be right. The hard work is not coming up with them, but to provide evidence. Franklin looked at the data and proposed the various possibilities based on that. She specifically pointed out the high likelihood of a helical structure in the first paper. But as mentioned, the measurement accuracy did not allow for a fully resolved structure. Nowadays, you wouldn't be able to publish a paper on how you think the 3D structure is, without getting sufficient resolution. Rather, you would need to outline the possible variations, though you could discuss what you favor. Again, reading Franklin's paper's and the Watson & Crick one side by side, one is to m e a proper crystallography paper, the other one is merely putting forward a hypothesis. Just because they pushed it harder doesn't make it better in my mind. What you describe is essentially taking imaginary leaps based on incomplete data. It is fine for building hypotheses, but providing evidence is so much more important. There are folks, including scientists but also increasingly influencers who built careers from overselling their pet hypotheses based on incomplete data. The most obvious offenders are in the health sector which is full of grift and overselling health advice and products mostly based on overselling limited biological data. It is a non-zero chance that at least one of those folks happen to be correct, but we wouldn't (and shouldn't) just take their word for it. Rather we should continue to collect evidence until we can tell. Eh, in his autobiography he severely downplayed Franklin's role. While he might have reconsidered his stance later on, I am not confident that he would have recognized her contributions around the time the Nobel came around. Incidentally, the Nobel Price committee had another serious issue with sexism a while earlier with a true titan in natural sciences: Marie Curie. For her first Nobel, she wasn't even considered until her husband refused to accept one without her as an equal partner on it.
-
In my mind it is in some ways even worse. When I read his paper as an undergrad, I could not shake the feeling that I just didn't get it. The paper was fairly short, didn't really show any data and the "only" remarkable thing about it, is that he was actually right. However, in my mind this is not how science should work. We have to show data and demonstrate that the conclusion you arrived at is the only one possible. That is what well designed experiments are for. Or, at minimum present the possible answers based on the data you were able to generate and discuss those. Yet the original paper by Watson on Crick doesn't really do that. It mostly proposes a model, based on one possible interpretation, based on the data Franklin generated. I really never reconciled that feeling until at one point I was dabbling in crystallography and dug out Franklins' criminally paper (which was cited only a fraction of Watson and Crick's paper). There I found clear as day that the resolution they had was simply insufficient to clearly rule out confirmations other than the B-form. Franklin in her paper makes it really clear and proposes the right-handed double-helix as one of the possible configurations, which IMO was the right call. IOW Watson and Crick they had the right idea but didn't actually put the work in to provide evidence. They just postulated it and happened to be right. And this is one of the things that is a problem in science, that folks that are considered "towering" can make calls without having the evidence (or even putting their own time into it) and are declared heroes when they happen to be right (and often just conveniently forget the times they weren't). Other folks, especially women, or other in the old boy's club OTOH have to work harder for less recognition. It took me way too long to realize what I didn't like about the paper that has been lionized and that realization has sufficiently soured my view on Watson as a scientist. While I never met Watson, I have met folks who were a visiting scholar in his lab. Suffice to say that there was nothing that really there that could have improved my view on him as a person, either, even before the allegations were widespread. In a broader sense, it is emblematic for the desire of folks, including scientists, to have visible rockstar researchers. Lionizing those rarely benefits science and more often than not it takes away oxygen (and funding) away from those that are doing steady work without overselling it.
-
Also, it will be the drawer that jams shut because your tongs have cross-linked with your pliers and decide to hold down the fort until kingdom come. They also seem to multiply and I might have to give up on the kitchen entirely.
-
From a quick skim, most examples refer to specific mechanisms that have been selected as a part of co-evolutionary process. Allergies seem to be more linked on an individual (developmental) time scale.
-
Yes, to some degree, but I think "pollutants" leads things a bit astray again. What is being argued in the paper (and a series of other papers) is that the exposures are more dynamic interactions with the environment, including microbiota. Importantly, these are likely not point exposuires. And instead of pollutants, one might thing of them as biosignatures of the environment the children live in. I.e. by continually being exposed and interacting with biomolecules in their environment, the immune system is learning about what is a regular/normal situation for the child. It should be noted that this could include potentially harmful exposures and I think the jury is still somewhat out whether that helps in the long run or not. Cool, does he also have seafood allergy? I know a great sushi place!
-
Good paper. Most is conjecture (based on evidence) but is more certainly more coherent than the hygiene hypothesis. I also like the fact that they are not overfocusing on the gut biota. While relevant, IMO it dominates the view too much, because there are just so many folks working on it and not because other factors where shown to be less important. For example, I think that the environment/immune interaction at the lung level is still understudied, mostly because it is very inaccessible compared to just looking at stool.
-
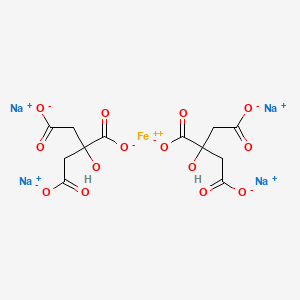
Hmm that is odd. Most ferric compounds are somewhere in the spectrum between black and yellow. The only whitish ones I can think of are some form of ferric sulfates as powder (white-yellow) but in solution it turns reddish brown or at least yellow. Does something precipitate at all? I wonder if it could be another metal...
-
That certainly looks compelling.
-
Could be this: In turn, I couldn't find a good picture, but in my memory it was less a bright green but more brown/grey-green-ish. But entirely possible that I am confusing compounds, it has been a minute. To make things really visible you can also shift the pH (e.g. using NaOH or if not available baking soda). In presence of oxygen and pH >7 iron precipitates rapidly in form of insoluble ferric oxyhydroxides that should settle quite nicely.
-
Upon reflection, I actually don't think that regular meal times are that unusual. I recall a practicum that I had where we looked into feeding patterns in birds, based on dominance patterns. IIRC, the birds we investigated typically had two major feeding cycles, a bit early in the day and late before sleep time. The assumption was that they kept lean most of the day to avoid being too sluggish, but less dominant birds in a group would feed more frequently as they were less certain to get something from the feeder. Considering that in most animal species feeding patterns are driven by the circadian clock (there exceptions, like predators who digest their prey over prolonged periods) it is likely that for the most part their feeding pattern has some regularity. In general, the pattern would match their activity periods (e.g. nocturnal vs diurnal), ability to store or acquire food and so on. Evolutionary speaking, it makes most sense the molecular mechanisms regulating hunger (and drive feeding patterns) are in line with the environmental pressures and opportunities that would allow food acquisition and there are strong interconnections in prey-hunter relationship of these patterns (which is what the practicum was based on). I think humans are not so special in that regard, except that in industrialized nations the food supply is not a limiting factor anymore. Instead food patterns are a compromise between natural predilections (i.e. feeding at least once a day, and usually during the day) and the requirements of job patterns.
-
I am a bit rusty but from memory, ferrous citrate was gray-green, but more on the dark grey side. Ferric citrate would be more on the brownish side. That level of green does remind me a bit on ferrous sulfate.
-
Hard to tell from the picture, unfortunately. I'd expect Cyanobacteria growth to be gradual and this looks like too much to happen overnight. Plus, generally they need a pH of > 6.5 to grow well. Is it settling on the bottom?
-
To be honest, I did not notice any typos. I frequently don't find my own to begin with. Regarding regularity, I don't think that this is universal in humans, either. In many cultures, it is heavily determined by seasonal activities. Those dependent on hunting, would often have meals after a catch, which can vary. And in a meeting with First Nations Elders, the typical meal times were described as one element of colonization, as traditional in some First Nation cultures, their mealtimes were more flexible and dependent on hunger. I strongly suspect that some of these patterns were dependent on how regular they have access to food. Seasonality was a bit thing too, as it determined what food was available and how long it would take to acquire it. Nomadic cultures can have communal meals in correspondence with their traveling patterns, whereas groups with a more agricultural component might have more regular patterns. Depending on time and place there are various constraints, e.g. availability of natural light, how easy it was to make fire or other meal preparation methods and so on, that I find it hard to believe that regularity was very common or even easily achievable until a number of developments happened, such as settlements of a certain size, predictable availability of food, improved food preparation methods and so on. So only off by 200 years or so ;).
-
I think it is way more likely that it is a behavioural pattern which developed when cooking and other forms of food processing became a key element of human dietary habits. Creating a cooking place make things less flexible and more efficient to do it more centralized with fewer times a day used for feeding. Many groups which rely on hunting tend to have 1-2 meals a day, but there is also eating throughout the day when they have plentiful access to preserved food. Also, it should be noted that while feeding might be regular, the timing might not be and depend highly on food source and related to e.g. hunting patterns, seasons and so on. I think that specifically three meals a day is a rather modern development and I wouldn't be surprised if it was linked to the rhythms created by the industrial revolution.
-
Most likely the formulation contained spores. The toxin itself can be deactivated by cooking, and Clostridium botulinum itself is not terribly hardy and it is an obligate anaerobe (i.e. does not survive oxygen). Spores, however are fairly hardy and can survive drying very well and are fairly heat resistant. They can be inactivated by prolonged autoclaving and potentially heating for an extended amount of time. However they usual inactivation times typical for bacteria which are required for food preparation, will be insufficient. Most likely, sufficient spores survived the process to cause infections in infant guts (but I would need to read up the reports to see what was actually found). Unlikely, the production requirements should be identical.
-
I think one of the original ideas is that if set up as non-profit, they would be sustainable, but not profitable. But from what I remember they made significant losses. What I don't remember if whether they managed to address the challenges of food deserts. I.e. whether e.g. local and especially low-income folks were using them (or could use them). Somewhat independent of that some food banks have started to set up grocery hubs, essentially free grocery stores like other food banks, but giving folks more of a grocery experience in order to promote agency and reduce stigma. But of course, it is an entirely different idea. That is one of the things I am looking most forward to. That is, an alternative to unlimited power due to unlimited money.