FreeStyle
Members
-
Joined
-
Last visited
-
Long story short to avoid useless sophistry... The references for that AI statement exist in the online realm, I am just curious how they were measured: https://pmc.ncbi.nlm.nih.gov/articles/PMC8766623/ Where did you see this recommendation? I keep seeing it on pages that need to make sales or are funded by such companies, which isn't always bad, except when it is. What other processes are you thinking about that don't seem to be affected? Just Vitamin D synthesis? There are a lot of sunscreen ingredients with potential for endocrine disruption: https://academic.oup.com/ieam/article-abstract/17/5/940/7727851 I personally for example use sun cream only if I know I will be in strong sun for more than 1 hour, but with an acquired tan I only really apply it on face neck and shoulders, and then on areas of the body with moles, and I won't do that each time, just because I think it wouldn't matter a lot, maybe I'm wrong. Overall, I prioritise vitamin D intake, which is low in countries such as the UK. Perhaps this is important to specify, because of my skin colour, which because of my genes can go from the standard inbetween type I-II to type IV (dark olive, or even darker) without much headache, which I can only do because I afford to relax in the sun even during the day because of my working arrangements as opposed to an office worker, and additionally, as I am not an average Caucasian in the Tenerife summer in my habits and observations. As a rule of thumb, I will not try to draw general conclusions of how much A Danish person burns or synthesizes vitamin D on a week in Sicily, if you understand what I mean. What you need to remember is that if your test group has Type I skin which does not seem to go olive with sun exposure but bright red, the sun may not only be too much, but they've either very nordic in genes or have genuinely not been exposed to the sun throughout their lives or past few years (scinency lingo? their melanocytes have not been stimulated). Depends on how much you were taking, I was told by a few doctors that 1000 IU and 2000 IU are recommended daily especially if coming from a sunny climate, which, of course, would have been hard for our ancestors to obtain over winter unless they had nice fat stores, as vitamin D is also stored in fat. Have you done a blood test to see how much plasma vitamin D you have during winter or summer? https://www.health.harvard.edu/staying-healthy/the-science-of-sunscreen "Q. Does everyone need to use sunscreen? I've heard some people say that they don't need to wear it because they have darker skin that tans well. A. We recommend sunscreen for skin cancer prevention, including melanoma prevention, which has been demonstrated in cohort studies as well as prospective randomized trials. Given that darker-skinned patients have a very low risk of skin cancer, using sunscreen for skin cancer prevention is not necessary. However, people looking to ward off the aging effects from sun would still benefit from sun-protective habits, which include sunscreen, sun-protective clothing, and sun avoidance." The loss of nuance is strong, yet it is clearly observed. The article does not specify, but quite obviously, "darker skinned patients" are not just the passively darker ones... this darker skin is also, very importantly, obtained through exposure. It is quite important to not be virtually transparent (it's a joke) when you step out in the summer sun, like so many people from northernmost countries do for absolutely no reason other than being silly and not caring, as is to not burn yourself (or chop your fingers off - some things are a logical given). It is rather detrimental to your pocket and health to always be lathered in cream, assuming you do what most people do by mistake due to sweat and other factors, such as getting it in your eyes, nose, groin, or eating it by mistake because you wiped your forehead before eating, because chemicals bioaccumulate, and they are everywhere around us. It is useless to analyse just one ingredient and say "swallowing this from this source is not going to harm you" because it simply means that item only, and you may still have everything else with dodgy ingredients in them. The BAD article links to this: https://pmc.ncbi.nlm.nih.gov/articles/PMC6899952/ Let's analyse it quickly, though. They analyzed serum vitamin D but do not tell us anything about their diet or supplementation, both of which contribute to vitamin D serum levels. The error factor of this alone can be anywhere between 1-20% or over if anyone was supplementing or consuming a lot of oily fish, as for example we also know some people consume things like Huel, smoothie powders or fish oil pills which tend to have vit. D added. We can assume they did not overall, it's what I would assume, but I also do not know enough about their possible diets in Tenerife to infer it, all I can do is hope they considered it. Factor 2: The control group did not go to Tenerife, but stayed in Poland. The countries have vastly different UV charts... My problem with Tenerife is the principle of the study. Being by the seaside in sunny weather and above 20 temperatures gives you excess vitamin D the body doesn't actively use. I read somewhere (and you're welcome to try and find such info) that 2 hours by the seaside in sun, in skimpy bath suits, gives you the equivalent of 10,000 IU. Blocking Vitamin D may be significant if your vitamin D levels are borderline, and you cannot afford to run naked on a beach, on the other hand. Modifying factor number 2: They were not followed by the team of scientists on whether or not they kept applying the cream on all the time... I'd assume most people wouldn't apply it all the time unless they were scientists themselves. You all need to go back to the maps I linked, showing a clear trend. As we know, the reality is better than random studies with highly variable control factors, although they do remain useful and interesting for society nonetheless. No one here really tries to explain why higher UV and olive tan do not correlate with high skin cancer rates. Suncare use by buying power does not correlate with lower cancer rates either in developed countries... although we should assume that's because it is also applied improperly. Now, I explained to you why, my logical theory.
-
My brother, you need to read it again because you did not understand it. I copied the AI paragraph to question it, not to provide it as a reference for my words, hence why I'm asking quite clearly at the end if anyone can help provide the original reference to it. As I answered in my reply to pinball, melanin production is a result of skin exposure to the sun, and lack of melanin in strong sunlight is the number one reason for burning, as observed in patients with extreme lack of melanin such as albinism or vitiligo. However, I want to underline that the way I word these posts is to learn, not to push a reality, or come across as a jerk that imposes its theories on others because 3 studies say so. To start the conversation by drawing a circle in a territorial manner is to, essentially, end it prematurely. Some things I write are obvious to me whilst some are not to you, but you may need to search the baseline yourself if you did not know or are completely unfamiliar with that, essentially. I hope I don't come across as accusing you of "ignorance", the only thing is I'd appreciate if you could contribute with some theory. If for some obscure reason you might be averse to all of that, then I assume you won't read a fully-fledged study, so, here I am providing something, just scroll to the conclusions: https://pmc.ncbi.nlm.nih.gov/articles/PMC2671032/ that is from 2009, when they were observing that "subjects with White skin are approximately 70 times more likely to develop skin cancer than subjects with Black skin" however, the European-level incidence of skin cancer suggest that we don't need to be of such drastically different origins to observe statistical differences... The study also shows microscope pictures of what melanin looks like and is. If you would like to help/contribute with a study that's younger than 6 years, please do. I believe salon bed tanning habits is probably not having a big influence on the overall numbers given the low number of users compared to the general population, although perhaps incidence of skin cancer is higher among sunbed tanners, as we'd think logically? Otherwise, this is good at explaining what we think melanin does and how it protects the skin, not just as a barrier, but as a free radical scavenger, which studies that only measure SPF will miss: https://www.nature.com/articles/s41598-024-53941-0. However, it also questions whether other independent factors might affect the degree of sun protection granted, other than melanin. If skin cancer mapping clearly shows a preponderance of such disease in countries with the least sun exposure and skin melanin, but you've got in-vitro studies concluding everyone should use sunscreen and they didn't find skin melanin to be important, is it probably worth questioning those studies and their sponsors? and if cancer prevention is enabled by other factors than melanin? So far, according to most studies, it seems that melanin has the highest protective role, and there is not much to indicate otherwise. "Skin pigmentation has been considered the main photoprotective factor against UVR, and ionizing radiation, with many epidemiological studies showing a lower skin cancer incidence (20- to 60-fold) in dark skin (skin type VI) compared to light skin (skin types: I–II). The risk has often been attributed to differences in the content and composition of melanin in the skin. Melanin, a complex biopolymer with condensed oxidized tyrosine as basis, is the most abundant skin chromophore, being presented as dark eumelanin and reddish pheomelanin. Melanocytes synthesize and package melanin in the form of melanosomes and transfer it to adjacent keratinocytes, where the pigments arrange perinuclearly to protect the skin against UV-induced cell damage. The distribution of melanin in a capsular structure over the keratinocyte nuclei is required to constitute a physical barrier that scatters, absorbs, and thus, reduces the penetration of UVR through the epidermis. It is well known that photoprotective properties of melanin derive from its broad absorption capacity in the UV–Vis range, together with its antioxidant and radical scavenging properties." I would like to add that with a lifetime or years of consistent sun exposure, melanin will persist in the skin even in skins type "I and II" as used above, even throughout periods of no sun exposure when the skin would otherwise return to its lower melanin content, as I have personally observed in families with older individuals who were farmers or spent a lot of time outdoors vs siblings or other relatives who didn't. Additionally, I posted those maps to ask users what they think of those trends and what could drive them, as my opinion/theory is, basically, due to melanin production through sun exposure, because people in those areas have normal white skin in winter, but the capacity for "tanning" (melanin production) is quite high in the general population, but only granted with sun exposure (otherwise, generally, people will still burn with sudden exposure to summer sun in Romania, Greece, Spain, etc.)
-
I wrote it in the original post, lack of melanin in strong sun is extremely damaging to the skin, otherwise noticed to an extreme in albino and patients with vitiligo. Melanin is what protects it, but the only "safe" way to obtain more of it is through sun exposure, which is ideal when the sun is mild, to begin with. I think most of us on this forum do, but it has been quite an efficient tactic throughout the years for people from my circles, aka progressive tanning. It's the natural way. Overreliance on sun cream is intense right now, too exaggerated exactly because people don't go out anymore because they think "oh no, the sun is cancerous because it shoots ghost noises radiatioooon 🤯", and that's just pure fear-mongering. Sooo... maybe, how light do you mean? Pink? lol :P As a side note, China, Korea and Japan have disproportionately high numbers of sun avoidance exaggerations like that. I do not think that is true. The research I linked says it didn't manage to show any correlation between occasional sunbathing holidays and melanoma incidence. I'd also add that most of the population were farmers, and although they'd try to make their lives easier, they'd still have to stay out in the sun A LOT compared to us, because of the nature of their occupation and need to connect to people or reach out to them, though it may be that men got out more than women. Women, due to the Churchly beliefs and other social practices, were likely kept indoors more? Yeah, there are a few different statistics on the lines of: -detection rates -who dies more from them -who finds them more often but escapes alive With low healthcare access seemingly still not even denting the big Nordic figures otherwise present
-
Ah yes, the typical "if it's commercial, I'm sure it's good. I will look into this no further". I was using a coal tar shampoo from Neutrogena sparingly and, recently, when trying to find it on the shelves, I discovered they weren't commercialising it anymore. Their website says it's because it wasn't safe to handle anymore, but apparently the lawsuit covers the customer side too saying the concentrations weren't low enough to not have any carcinogenic effect (with regular use, I assume, or when used on children or pregnant women?). And that proves that things like this happen often enough. Another ingredient that has been found recently in too high quantities in hair products has been benzene. And, give me one big second. We are talking about US/EU here. Good luck to you anywhere else in trying to find stuff not contaminated with heavy metals.
-
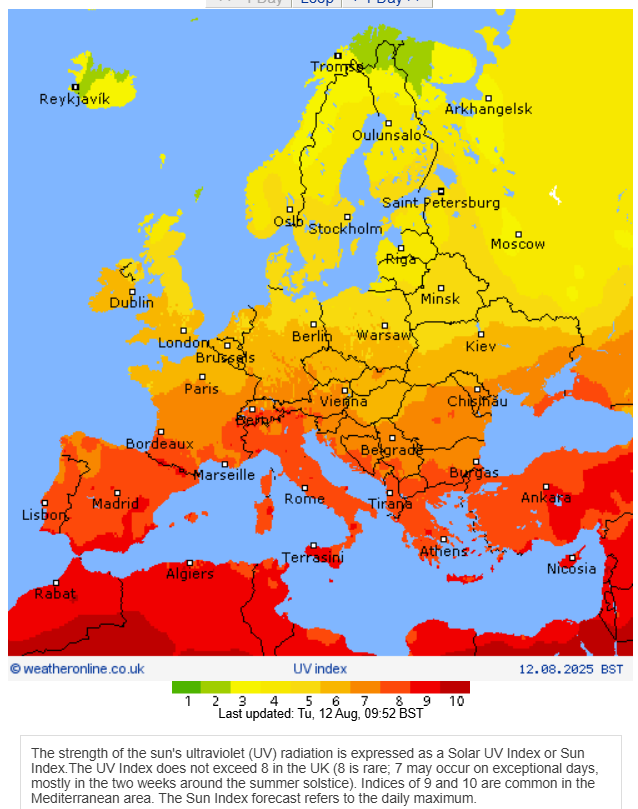
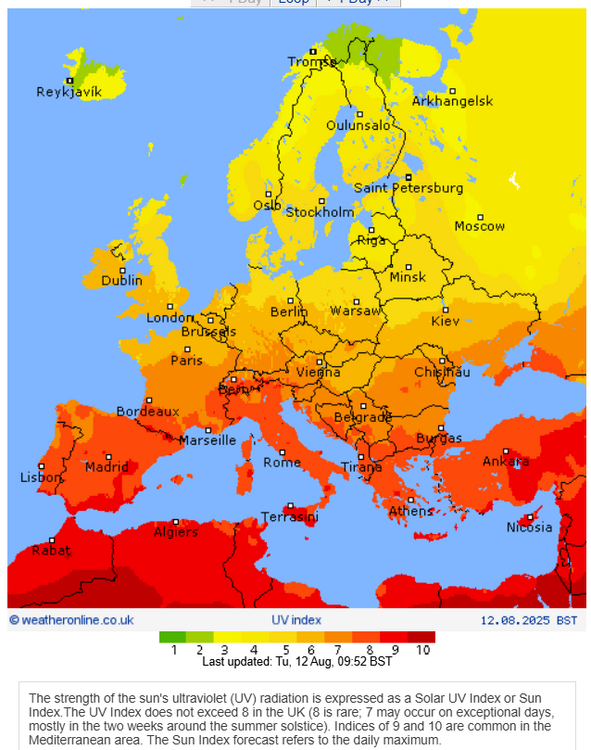
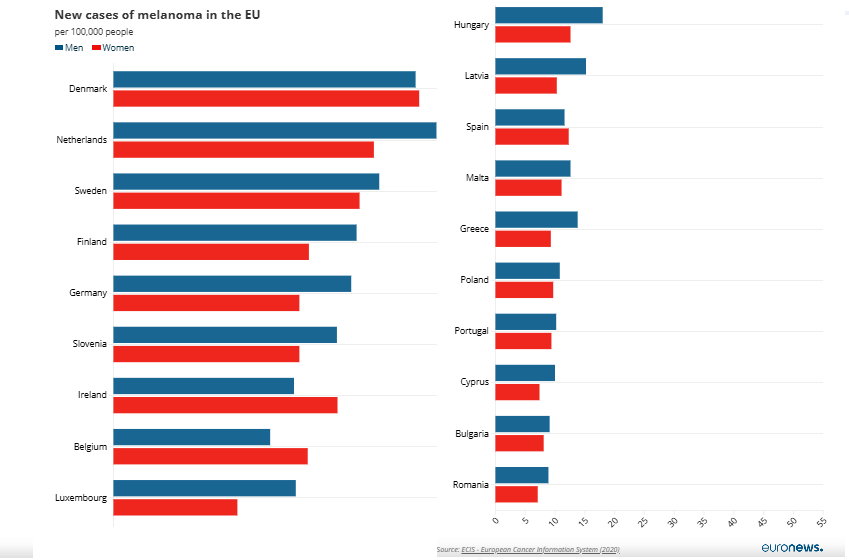
I would like to say that I am opening this topic because it is tiresome to interact with the online fear-mongering about SUNLIGHT. Even when it comes to gradually exposing yourself to sunlight, the push is to instead swallow vitamin D pills. It is mostly touted in cosmetology and dermatology, and the internet is chuck full of this content aimed especially at women. Whilst it is still a good idea to apply some basic skin care as an adult, in areas with high UV radiation and not only, and especially on the face, neck, and shoulders, I feel like it's gone too far. (As, for example, overall in Europe -which isn't the best statistic for an individual person but here we go - there are less people dying to skin cancer ~around 15k~ than due to car accidents ~around 20k~). The data is pretty clear. Skin cancer (which includes basal cell carcinoma, squamous cell carcinoma, and melanoma) is largely caused by UV radiation, especially UVB, although other contributing or enabling factors should naturally not be ignored, should you be subject to these (such as a weakened skin barrier, like during an active episode of psoriasis). Despite that, the countries in Europe with the higher UV indexes -> -> such as Romania, Bulgaria, Greece, Cyprus, Malta, all get significantly lower skin cancer rates than their more northern brothers (Denmark, Ireland, Sweden, Netherlands), despite people's purchasing power being significantly lower. https://www.euronews.com/health/2023/07/19/skin-cancer-which-eu-countries-have-the-highest-melanoma-incidence-and-mortality-rates North America, New Zealand, Australia, all are chart records in terms of skins cancers https://www.sciencedirect.com/science/article/pii/S2949713224000582 , and something much less discussed is these countries is that they are populated with a type of people that did not evolve in those UV areas of the world, with frequent genealogy tracing back to Irish, German, British, etc. settlers, with not just low epidermal melanin, but also habitually less exposure to sunlight especially nowadays. Arguably, people in countries like Spain, Greece, Romania, etc. have higher melanin and "capacity for tanning" even when starting off from the same "white-ish" baseline (for example, a long winter) as an environmental adaptation. And that's what I wanted to point out. Gradual exposure to sun (don't burn yourself until the skin peels off) is more beneficial than hiding under umbrellas and 3 layers of sunscreen because you're milk-white in the middle of August! That kind of avoidance is more dangerous. Agree? There is a point I'd like to discuss, which is the following AI statement on Google: - "Darker skin tones, with more melanin, have a natural SPF of around 13, while lighter skin tones have a much lower natural SPF, potentially as low as 2-3. However, these natural levels are still far below the recommended minimum SPF 30 for adequate sun protection." Have you found the study indicating the measurements of 30 "SPF"?
-
Honestly, I think I can only make a limited number of posts because of being new, so this is going to be a postzilla thanks to... you'll find out :)). Considering you have 4 posts all reference-less in here, and although your valiant request for references is good for research-heavy circles, it's rather odd you seem to stay away from them yourself in the context of this topic. In fact, I simply took you as an example for my first post. Going back to the subject this topic seems to tackle, it's referring to two very complex problems, different from each other, aka infant mortality rates and adult mortality rates. Is does not distinguish much between post-Black Death deaths and pre, or leaves it to us to do so. It's like analysing the Nahuatl-speaking population, or those around lake Texcoco for deaths before and after the Columbian "sojourns" (conquests) and his tasty germs. Important distinction, as we may as well look at infant mortality right now in UKRAINE. And dating burial sites with less than a "50 years window of error" is difficult. Referring to just the British Isles' gentry is limiting our ability to generalise, which the title does, unfortunately, but is a good starting point given the written evidence that exists... moreover, some of the people here seem to confuse the terms.: some research papers refer to "at birth" whilst including the whole first year of life. Some exclude stillbirths, which shouldn't be completely excluded imo if they were late pregnancies. And you know what no one wonders about? Intentional infanticide. There was little safe birth control, if none for many, other than abstinence, spermicide/contraction herbals, or the not dangerous at all stretchy animal intestines like we do nowadays for sausage casings, except not for the kind of sausages you're thinking of. And for accidental pregnancies, the undesired children did not fare well, and might've been killed off. It doesn't seem unusual at all to consider that Medieval people, with all their woes, might've also ended the life of a sickly or malformed child to give better chances to the next (or existing ones), either passively by neglect or actively by physical means. The Ancient Greek historian Plutarch wrote about the society-wide practice of the Spartans "any child that appeared defective was thrown from a cliff of Mt. Taygetus, to die on the jagged rocks below". Though this is still disputed, it's not hard to see why people might've done it when they lacked the conditions to keep a premature birth alive - even when considering that the presence of the Church likely made this more difficult in Medieval England. Neglect happens nowadays too A LOT to unwanted pregnancies carried to term, or if a parents gets ill. (You can easily see all the neglected children congregating on reddit these days oO) cough jokes aside: Death is multifaceted, and pollution tends to be slow, not swift, and, on a snide note, will become faster-acting depending on how much longer environmental regulations will be taken as a suggestion rather than rule. In fact, it is highly likely many people died during Medieval times due to sewage pollution as we'd now call it. Indoor cooking and exposure to fumes and particulate matter likely contributed to earlier deaths as well, particularly due to the UK's poor climate (wet and cold) which forced cooking indoors and with improperly cured logs (wood likely to still hold moisture); but also due to molds. Speaking of cooking fumes: "For billions of people across the developing world, particularly children and women, mealtime starts by firing up a kerosene stove, lighting a charcoal grill or setting some logs ablaze. The problem: much of this cooking happens inside and the smoke it produces is laced with toxic particles. This type of household air pollution led to 3.1 million premature deaths in 2021." comments the UN https://www.unep.org/news-and-stories/story/cooking-smoke-kills-millions-every-year-heres-what-world-can-do-about Immediate or identifiable pollution-attributed direct death is low in the general population unless they live close to spill sites, are influenced directly by a large pollution event, or work with, say, coal tar... and few people suggest otherwise. What pollution does is reduce quality of life and make it easier for the manifestations of disease/imbalance to form in a way we can identify, such as cancer (see the thyroid cancer rates in Fukushima and nearby fishing villages if they show that too https://pmc.ncbi.nlm.nih.gov/articles/PMC5770131/); or the deaths attributed to cardiopulmonary arrests and cancers due to air pollution with particulate matter (but not only) from coal burning in Ulaanbaatar https://pmc.ncbi.nlm.nih.gov/articles/PMC3578716/. Although this pollution was measured mostly in PM2.5, you should know pollution is measured in more ways than this, including ground-level ozone, but they just needed to prove a point swiftly. P.M. itself further differs in chemical composition depending on where it comes from, with the oft radioactive coal not being a great source to inhale from compared to pollen for instance - I hope the ironic use of "not great" is obvious - , as pollen also breaks down to a size of 2.5 as a P.M.). As you see, we could be here until tomorrow if we delved into topics how you think we should, but very few do (this sentence is aimed at some two posters above me who did not like the lack of Googly woogly references). In any case, it seems to me like most posts actually agree with each other that the cumulative knowledge of medicine and the world around us has put us in a better spot than before when it comes to infant mortality rates, so I'm not sure why people get so upset at each other for. L'amour de l'art de la polemique. In regards to my observation of the impact of STDs and STIs in infant mortality rates, I don't know... you make a good point to remember about HIV, but just because you've never heard about the rest, doesn't mean you couldn't google it for 5 minutes and then claim it's non-scientific... it's really not such an incredible comment to write. STDs and STIs, which existed in Medieval England, that can cause and likely caused infant mortality, either soon after birth (within the first year) or due to miscarriage, included syphilis, gonorrhea, HPV, hepatitis B/C, chlamydia. They still do sometimes nowadays too, but since most of those are bacterial, we can cure them with antibiotics, and for the viral like the HPV, there are vaccines offered in the UK. https://pmc.ncbi.nlm.nih.gov/articles/PMC9302697/: effects of chlamydia, gonorrhea, and hepatitis C on infants are significant, from association with low birth weight to being born stillborn or calling for C-sections (which the Medieval Ages didn't really have; and which effects or deaths, like back then, may also just be caused by poverty-associated issues). Whilst the numbers of such deadly infections on fetuses remain low generally, that is because the study was done in 2022, when infant mortality had been greatly reduced to just 1-2%! (this surprised me too for that area of Brazil. Anyways, if you check the Nuffield Report 2018 on infant deaths 2017 vs 1948, it's the same for England, even lower death averages in general) https://www.scielosp.org/article/csc/2025.v30suppl1/e16642023/en/ Unfortunately, due to limitations in not just funding but also surviving archaeological evidence, only the more destructive ones like syphillis can be more accurately identified in bodies after death and decomposition due to the disease's effects on the bones; and this means that this one ended up being the most studied, or amongst the most studied. Surprisingly, and simply throwing this here because now unlike the middle ages we have condoms that everyone affords to buy or get, Gonhorrea cases are rising compared to 1920 when much less people used barrier protection and there was no NHS in England (so was this data recorded accurately at all?), but the Spike's origin is suggested to be in the foreign-born population, which could or could not be true, https://www.bbc.co.uk/news/articles/c4nnmgzkgm3o + the different sourced chart below: As Smiths College points out, "Some historians have long believed that treponematosis existed in medieval Europe, but paleopathologists (who work with teeth, bones, and aDNA) lacked the evidence to prove it. Over the last decade, however, instances of skeletal remains with damage symptomatic of treponemal disease have appeared more often in the literature." For example, for King Edward IV's death, the chronicler wrote "that the king had died of an “unknown” disease not easy to cure even in a man of “lesser status.”" which is now apparently believed to have been syphillis. There is a lot of interpretation to be had when it comes to the centuries that passed and sometimes the best thing we have is our own rationality and knowledge. Unfortunately, it's chronic diseases that tend to leave traces on the skeleton. And all archaeologists many times have is odd description of Ungodly plagues, and bones. If modern day's burden of infant deaths attributable to sexually transmitted diseases and infections is at in less developed places such as... Florida... (*cough* xD), even this study (https://pmc.ncbi.nlm.nih.gov/articles/PMC8284346/) says "The lack of recent and national data assessing neonatal herpes mortality remains a substantial knowledge gap that this investigation aims to address." as well as "We are aware of only 3 US studies that characterize herpes-related infant mortality in a defined population" and it's also because I think we should all know how deaths are coded in public hospitals due to laziness, lack of interest or tiredness of staff... this I speak from genuine experience and friends from the system. if you want to believe that or don't, that is entirely your problem (whoever reads this) as I doubt any hospital would let me publish official statistics on their "malpractice" or "bad data input practices" without big funding going on. However, the Covid Pandemic has made this a point of discussion as "excess mortality attributed to COVID deaths when other co-morbidities might've, in fact, played a bigger role." Further on the nutritional difficulties of women who had to carry the fetuses (Uni. of Reading, Shapland F et al. 2016): "An average age at menarche of between 15 and 16 years would be much later than the modern British average of just under 13 years. In addition to their shorter stature, this finding adds weight to the argument that environmental factors such a deficient diet and disease were having a negative impact on medieval female growth and development." They go to suggest that "This may suggest that girls who experienced poorer conditions for childhood and adolescent growth were more likely to die around or before the age of 25 years." which would contradict the statement below that, sure, it arguably was discussing infant mortality, but the context as a whole also included adult females carrying them, dying: I mostly agree that it wouldn't have changed it a lot, if we assume people ended in poverty due to irremediable undesirable traits for those times such as learning difficulties, but it would've made a nice dent in our What-if exercise, should we assume poverty happened more by chance and was, to a certain point, undeserved more than anything else.
-
That's just because you're used to reading "scientific" arguments expressed in a cold fashion 😂 but this is just a forum, and I choose friendly expressions and minimal "references", though I have read my fair share of studies and articles. Your answer is very unfriendly, however. You made a point to dislike my exposition of words and from there, to just randomly disagree with every paragraph. Throughout your post you don't even debate, you just state, as if you hold all the answers anyway. Again that's not very nice, nor scientific. This isn't a contest of who is more of a smartass. I'm limited to only 5 posts today, so this will be my only reply to you 🙄. Fascination with STDs... Lol. Wtf? It's just an interesting fact not many think about that I put in writing. How can you say less travel only means less spread diversity, or ask me what exotic pathogens mean? It means pathogens exotic to where a person's lived (in the layman terms you so hate), as the OP did NOT give a geographical location for these Middle Ages, which in case you didn't know happened at different times in different countries... Low vitamin isn't "snuck" in there unless I'm trying to create magic spells, it's the reality of not readily having as much fresh available produce in winter like we do now, such as fruit. Or pills like we do today. This is a fact. Tell me the following: can you even read a foreign language to be able to understand estimations made on average lifespans in the middle ages in other places of the world? The fact that you disagree with life back then being very unkind to many individuals of "lower standing" and with the fact that many might've survived if say social stratification was less stringent in certain places like the british isles, is your emotional choice, not a scientific one. Such an unkind carrot in the arse post, honestly, and you're not even an expert on Middle Age matters in any capacity.
-
That's for sure the wrong answer. First of all historical observations can be skewed depending on source amd because they happened long before you were ever born. Words inadvertedly twist meanings with the writers' subjectivity and knowledge of life or lack of, as much as they help us to learn. Secondly, it is well known environment modulates gene expression, but we are also social creaturea. As such, it is inevitable that a person raised in a highly reserved and introverted culture will develop and take from the traita they observe around them even when they don't fit too well by nature, simply in order to exist as part of a group. Such would be obvious for an average Italian going to Japan for the first time, for instance. Just look at how many kisses and words interactions locals exchange in these two countries as a standard, or how loud they speak, how often they rouch each other (as all of these measures intro/extroversion) and you'll understand which one is more reserved by tradition rather than by individual nature (where tradition overpowers individual nature, at least when it comes to public displays).
-
I of course don't hold the truth, but in my approach I use a combination of emotional and scientific knowledge (or perhaps we can call it experience too) It wasn't horrific by evolutionary standards. Some of it was probably needed because some of those babies were weaker and/or had difficult health issues for their times! It really depended on how good the mother's instinct and social standing were, to feed herself well and choose a... non-consanguineous mate, and shield herself from diseases such as sexually transmitted that even today pose problems because they're transmitted via placenta >.> Why people died so early? Stress, more diseases, improper nutrition. The lifespan nowadays is the way it is because we can prolongue life in a chronic illness state. Otherwise, our current lifespan averages would still be lowered considerably by those people who do not keep themselves well and develop diabetes, hypertension, obesity, alcoholic liver diseases, pancreatitis, etc. (first 4 are lifestyle diseases), IF we took their statins and etc. away (aka the "modern" life prolonging element in our equations). However, now we can also do blood transfusions in case of accidents, and know more in general about the human body. We've also reduced all kinds of violence in our society, assuming we're all from countries NOT at war... Bacteria and viruses: first, no, there were less species of these because people mingled and travelled less, so the strains had higher local specificity 🙂. It's highly likely we are more resistant now to more exotic varieties of viruses and bacteria, but less resistant to local bacteria. Secondly however, yes, in the sense that the idea of disinfection did not exist as such... People ate with their hands, bathed when they could once a week if they could, and STDs were everywhere. But there were less people in general, so smaller numbers touched the coin that ended in your pocket for instance. Infections and low vitamin intake killed lots of people though. From respiratory to flesh wounds. Antibiotics did wonders, but now we have the problem of evolving bacteria to resist antibios. What do you think?