


invasive-feces
-
Posts
21 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Posts posted by invasive-feces
-
-
What are the RT-PCR test results ("standards) with respect to Ct in various countries? (E.g., USA such "high" cases but China, India not so)
And does the Ct variation among different nations reflect what we see on the Johns Hopkins COVID-19 site?
0 -
Please discuss (list) non-antibody protection against pathogens like coronavirus.
The protection thru which tradit. AB testing may be ineffective or erroneous in CONCLUSION. In other words, COVID-19 may have gone thru an indiv. asymptomatically ... been "dealt with" by the indiv's robust protection/immune system. But when it comes to tradit AB test, the indiv. would be categorized as "never exposed" to Sars Cov-2. How common might this be?
Some this and other issues were raised on this recently-posted video. For example, immunity gained from NON-COVID-19 coronaviruses, etc:
0 -
About that COVID-19 scenario in 1347 AD (noted earlier) ... I maintain "not such a big deal" for addit factors such as:
- reduced population density
- no smokers (Tobacco)
- better nutrition (compared to std. American diet, processed foods, etc)
- far less obesity
- les polluted air
- sick people usually isolated to homes (not hospitals, with lots of potential vectoring); also, sick were shunned and discriminated against, evolutionary psychology's "bio-hazard" response
BTW: About antibiotics and pneumonia ... I agree that that is a huge factor for bacterial pneumonia, but I've heard conflicting reports on whether COVID-19 causes more serious VIRAL pneumonia. Correct?
53 minutes ago, CharonY said:And on the not a huge deal part, I should add that there is now significant evidence that even folks that recover from COVID-19 often show evidence of lung tissue scarring. There were expected reductions in lung performance, but so far it is not clear how much folks will recover.
New Scientist also reported need for extensive mental rehab, and possible permanent cognitive impairment due to the drugs/gasses they use to keep you either anesthetized and/or anticonvulsive while ventilated. (muscles and limbs can act up and cause you to do nasty stuff to yourself, like fall out of bed, pull out IV, etc).
0 -
4 hours ago, CharonY said:
1) is a misunderstanding. Prior to the the bubonic plague folks that reached adulthood were expected to live well above 60 years.
I don't understand this remark as pertaining to COVID-19.
Let's say, all else being equal, COVID-19 happened in 1347 AD. Over 60 age group were a far smaller fraction of total population than today. So COVID-19 would not be a "huge deal".
A modern analog may be occurring today in 3rd world countries. Not only fewer older folks there, but other diseases and ailments (as well as lack of medical care and nutrition) kill off the genetically weak in all age groups.
Rich, "modernized" nations care for the old and genetically challenged: Fresh meat for novel and opportunistic pathogens.
0 -
Said another way, via cliche, "whats wrong with this picture?"
 0
0 -
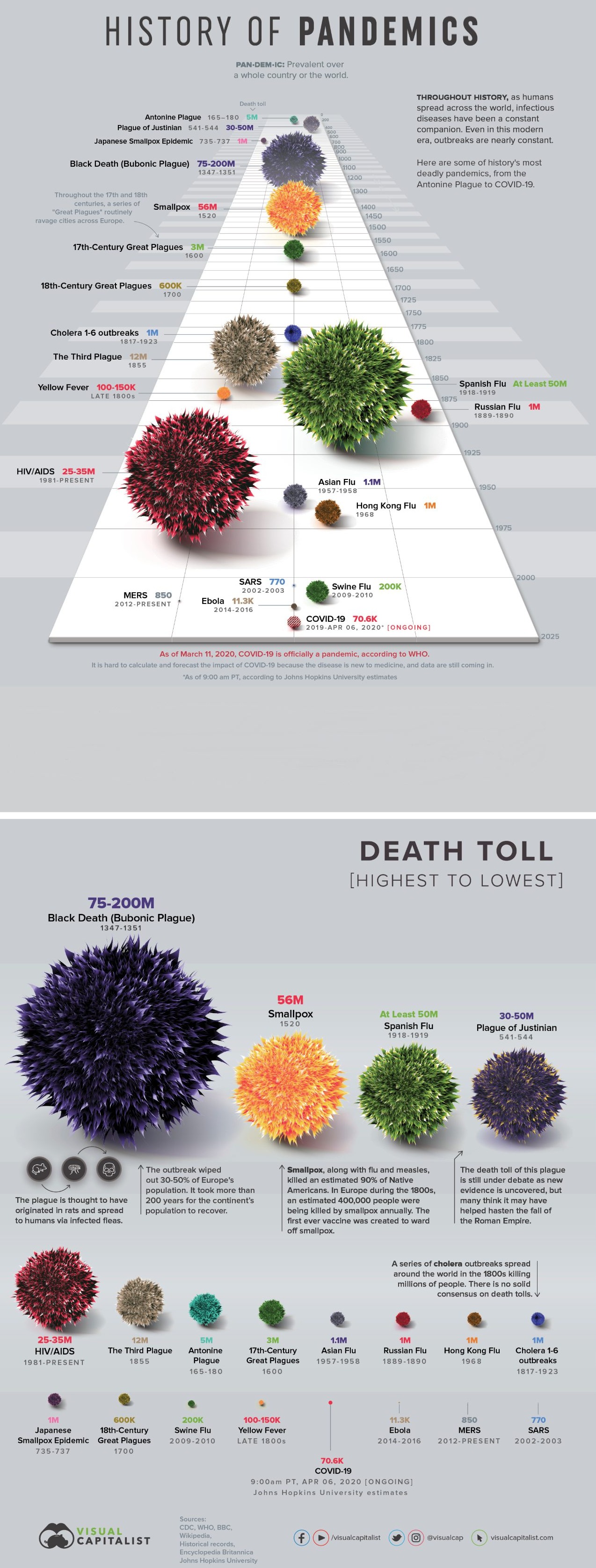
The following infographics were featured in the latest (June 2020) issue of Discover Magazine:
Large sized image of:above: https://images.ctfassets.net/cnu0m8re1exe/5Wcz9RvRq3yfnV6qWKvuZX/82d60cc1a74648e8c4b9819e2c112dff/Pandemic_history_copy.jpg
Concentrating on the second graphic (Death Toll; note COVID-19 data up to Apr 6, 2020), please list all the reasons why this presentations like this -- so common in pop sci -- may be inaccurate, irrelevant, sensationalistic, etc.
E.g.,
(1) COVID-19 deaths age group typically over >60yo (compared to Black Plague, when most people didn't live that long)
(2) Improvements in science, nutrition, communication (even compared to 1918 Spanish flu, when there were no ventilators, or antibiotics)
(3) etc. (add your own thoughts !)
0 -
About shedding and its temporality .... this Nature Medicine paper, about a month old now, seems to indicate Wuhan median = 20 days (max 37)
Temporal dynamics in viral shedding and transmissibility of COVID-19
https://www.nature.com/articles/s41591-020-0869-5
45 minutes ago, J.C.MacSwell said:Obviously that would be a concern, but if we can assume it can be sexually transmitted, let's say vaginally, would that give the body more time to adapt than breathing in the virus, given that this manifests most dangerously as a respiratory disease?
Introduce the word "sex" and it's like ringing the dinner for the media!
But the added sensational spotlight may not be such bad thing it prompts more research $$$ into medical SCIENCE
") 0
0 -
I just heard a report on Science Friday (??) that COVID-19 was found in semen. So it may be (or have become) sexually communicable.
https://www.webmd.com/lung/news/20200507/virus-found-in-semen-of-covid-19-survivors
0 -
I'm not sure much definitive info exits on COVID-19's "endemicness" in the open population.
That is, how long does this virus remain remain transmissible in any given individual (whether or not they became symptomatic)?
Can this virus "hide out" in an individual's system ... even for life (as in the case for herpes)?
1 -
38 minutes ago, CharonY said:
There is little relation between these observations. For influenza a challenge is that there are numerous strains and the annual vaccines are designed around the modeling of which strains migh be dominant. There are years where the predictions fail or when something really unexpected happen. Now SARS-CoV-2, has a significantly lower mutation rate than influenza. While different variants have been detected to since the outbreak, the changes were fairly minor among the dominant variants. Most vaccines target conserved parts of the virus which so far did not seem to vary much. However, there are other challenges surrounding the development of a new vaccine, of course.
So to re-iterate, I do not see any information from influenza vaccines that we could meaningfully translate to COVID-19.
Hmmm ... so both (influenza and corona), being RNA viruses, don't share too much wrt "recombination" ???
Let's say the current human-volunteer vaccine trials of COVID-19 do produce some positive results. Antibodies are isolated and a vaccine is developed. Are you suggesting this might be a treatment with, say, >40% efficacy (which is about the avg for seasonal flu vacc).
0 -
Are there any reasons to more or less hopeful of current expedited/heavily-funded/heavily-fast-tracked COVID-19 vaccine projects (being efficacious) when the CDC reveals the following stats re: myriad flu vaccine efficacy in prev season/years:
US Flu VE Data for 2018-2019 (note relatively poor %total effectiveness, esp in +50 yo)
https://www.cdc.gov/flu/vaccines-work/2018-2019.html
https://www.cdc.gov/flu/vaccines-work/past-seasons-estimates.html
0 -
I going to guess -- prove otherwise-- that most of the cases reported (recorded) are more from "dragnetting" operations as opposed to emergency-room walk-ins.
In other words, some one on a cruise ship, nursing home, etc. gets sick and is confirmed positive for COVID-19. And that leads to testing of that person's contacts and community. And many of those will test +, but be/remain asymp.
0 -
Anyone know how many of the positive (tested) CONFIRMED cases were/are asymptomatic?
E.g., as of today, according to
...in the U.S.A, there are:
1,384,033
How many are just " confirmed asymptomatic"?
According to..
European Centre for Disease Prevention and Control--An agency of the European Union
Confirmed case A person with laboratory confirmation of virus causing COVID-19 infection, irrespective of clinical signs and symptomsNot sure how many countries follow THAT definition.
0 -
Anyone know of COVID-19 stats for hospitalization (critical / intensive care, as in on life support)?
0 -
On 5/5/2020 at 4:42 PM, CharonY said:
I suspect the question is aimed at respiratory disease. I believe it has been asked and answered a few times, though knowledge is of course evolving. There are handful of studies who have tested COVID-19 positive patients for e.g. influenza, other coronaviruses an so on. In one study from Wuhan the co-infection rate was about 20%. In other regions such as Italy I have seen some higher estimates but with fewer tests.
~20%
https://www.cidrap.umn.edu/news-perspective/2020/04/researchers-report-21-covid-19-co-infection-rate
https://wwwnc.cdc.gov/eid/article/26/6/20-0299_article
0 -
Another co-factor to investigate would be seasonal flu shot vs. COVID-19 deaths (or serious CV19 cases). That is, might a seasonal flu -- even a very MILD case -- weaken one's defenses to "allow" SARS-COv-2 to "get in" and/or become aggressive?
0 -
The doctors in this recent interview do claim to have had patients with co-infections (but only mild CV19):
0 -
2 hours ago, CharonY said:
I suspect the question is aimed at respiratory disease. I believe it has been asked and answered a few times, though knowledge is of course evolving. There are handful of studies who have tested COVID-19 positive patients for e.g. influenza, other coronaviruses an so on. In one study from Wuhan the co-infection rate was about 20%. In other regions such as Italy I have seen some higher estimates but with fewer tests. The general consensus seems to be that it co-testing does not change clinical practice and is probably not terribly helpful with few exemptions.
Say an elderly person shows up at the hospital with a moderate case of pneumonia. Assume this occurs during the current pandemic in a state like Calif. That person -- because of his symptoms -- is tested for CV. And, yes, he tests positive for CV. But the person shows NO OTHER Covid-19 symptom. That is, the person is asymptomatic (or mildly symp) for CV, but is suffering from another respiratory disease. Maybe, given the man's age, the pneumonia will kill him. But the COD may be reported as CV19.
Hypothesis on this scenario ... how common it may be?
EDIT: I just scrolled a few pages back in this thread and found the co-infection topic already discussed;
On another note, might deliberately co-infecting the COVID-19 patient with another virus (say common cold) help somehow with build up of COVID-19 antibodies? Has anything like this been investigated?
0 -
3 hours ago, invasive-feces said:
Anyone hear of cases in which persons may be tested for multiple virus infections concurrently?
E.g. Let's say I got the seasonal flu and then COVID-19.
How common are multiple (concurrent) viral infections?
Let clarify a bit. Most species -- incl. scientists -- are probably walking around with multiple (non-serious) viral infections, day in day out.
Supposedly, 90% of humans are herpes positive.
That said, if a person with a seasonal flu also contracted COVID-19, how could you tell which virus was causing which symptoms? For all the cases of COVID-19 tested, were the subjects ALSO tested for other viruses?
0 -
Anyone hear of cases in which persons may be tested for multiple virus infections concurrently?
E.g. Let's say I got the seasonal flu and then COVID-19.
How common are multiple (concurrent) viral infections?
0
Lab animal pandemic/epidemic simulation?
in Microbiology and Immunology
Posted
Anyone know of deliberate (controlled) experiments to simulate some kind of infectious epidemic/pandemic in animals? Say, a whole building full of 1000s of lab rats or mice .... deliberately infected by some sort of virus.
Speaking of animals and epidemics or pandemics, anyone know of any important ones that took place in the natural or man-made world? Say, among house cats, livestock, etc.? Certainly, important-to-human animals are routinely vaccinated ... but is it with good, statistical reason?
About epidemics / pandemics of animals in the Natural world ... Yes, it would be hard to uncover / track that ... but has anything been formally recorded or documented?